I had been a Diabetes Specialist Nurse for 20 years or so, including a stint working as a Clinical Nurse Manager in New Zealand for 12 years. Then the opportunity to learn and grow in a new specialty presented itself, and I decided I was ready for a new challenge.
The trust I was employed by had had their first Getting It Right First Time (GIRFT) review in endocrinology. The clinical lead was asked by the review team/deep dive visitors what the first item was on the wishlist for the service and, without hesitation, his answer was an endocrine specialist nurse. With that, a part-time position was created, and I was the successful applicant.
With a very new position, and learning a new specialty within the confines of part-time hours, it has been quite daunting and, at times, a steep learning curve. However, the opportunity to specialise in a diverse and interesting field has meant that every day is a learning day, which most definitely provided the challenge I was looking for, and the next step in my career.
FINDING YOUR FEET

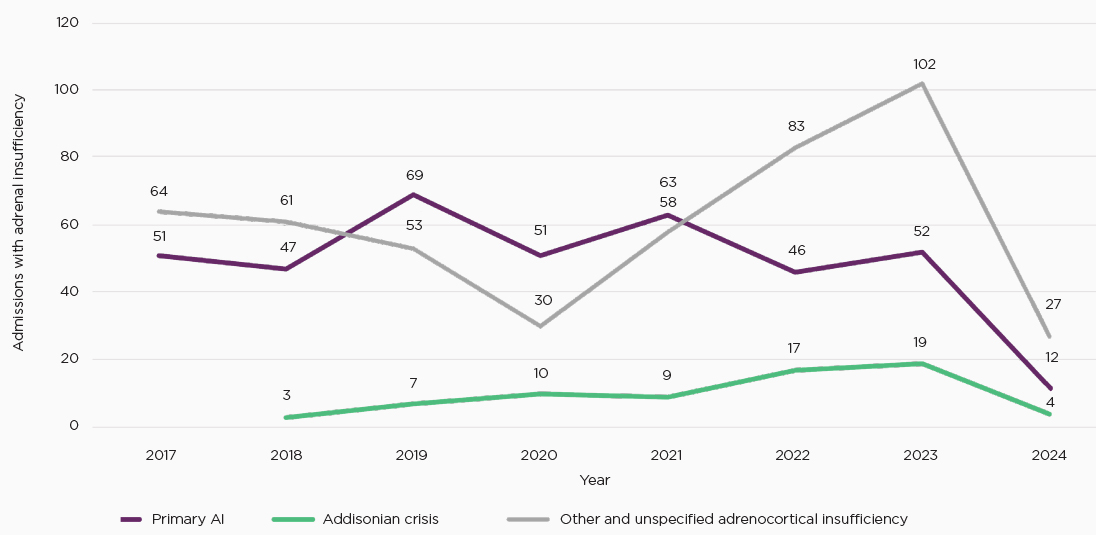
Figure 1. Reduction in hospitalisations for adrenal crisis following implementation of patient education programmes and emergency hydrocortisone kits.
New endocrine nursing roles, in discussion with other nurses, tend to consider what the local service needs are in order to support direct patient care. From a nursing perspective, I was able to start the service from scratch, as it was a new position, and I have been fortunate to have been able to influence and shape the service.
Two of the priority areas identified for the service were to establish dynamic function testing in the absence of a planned investigation unit, and to provide patient education for emergency administration of hydrocortison (see Figure 1).
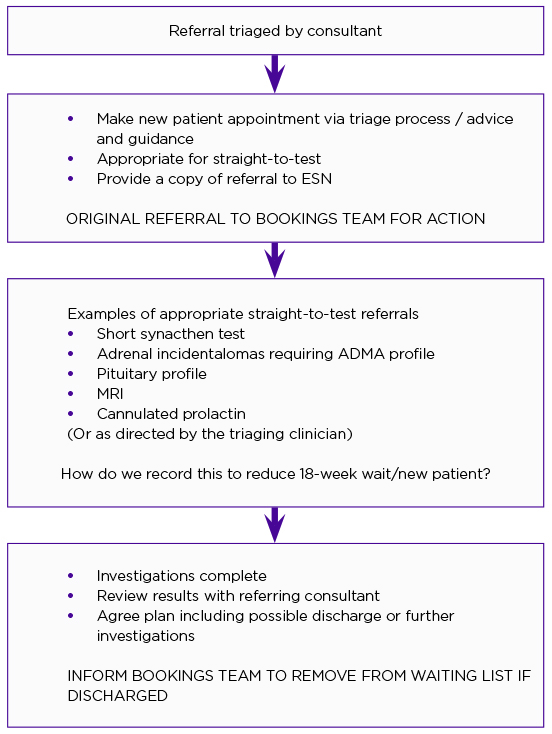
My candid first recollection (and somewhat naïve thoughts) regarding undertaking function testing was that I didn’t consider this to be part of my role. However, I have learnt a great deal about various conditions as a result. Slowly, some of the jigsaw puzzle pieces started to fit into place. It has also ensured that the journey of referral and investigation starts sooner, with improved patient satisfaction, based on our friends and family responses. I am able to help provide a diagnosis, including a timely discharge where appropriate, with the development of a defined pathway (see Figure 2).
Referrals to endocrine services have been growing over the past five years, with a 31% increase compared with a 17.5% increase for general outpatient referrals, based on hospital data (GIRFT).

Figure 2. Straight-to-test pathway, based on experience gained from a pilot run. ADMA, adrenal mass; ESN, endocrine specialist nurse; MRI, magnetic resonance imaging.
Straight-to-test involves proceeding straight to an appropriate investigation without a prior clinic appointment. The aim is to improve time to diagnosis, provide earlier reassurance, improve access to services and avoid unnecessary clinic appointments. This concept is well utilised in suspected cancer pathways. The GIRFT report (2021) highlights the importance of providing more pre-testing: increasing efficiency by making better use of pre-consultant appointments, the suggested target for services being at least 30%. As a result, endocrine specialist nurses can significantly improve the efficient running of departments. Time to treatment can also be improved and, as a result, so can patient satisfaction (Figure 3).
From a practice perspective, it has also developed my clinical skills. I understand the principles of investigations and have learnt to interpret results, including the next stage of the diagnostic journey to next stage investigations, including imaging. With time, I am learning how fascinating and exciting endocrinology is.
I have welcomed support from local services and endocrine specialists, with whom I have been fortunate to spend time. I know that if I drop them an email or a call they will provide support and offer encouragement, and they have been generous with their time. The endocrine community (who are fewer in number than the diabetes fraternity) are a friendly bunch, and I found it easy to contact colleagues through WhatsApp or the Facebook endocrine nurse group.
The Society has recognised the situation faced by many new endocrine nurses, as they tend to be singular roles, particularly in tertiary services. Support from the Society by means of the early-career nursing scheme has allowed me access to the online platform Qooper (www.qooper.io), where I can track my competency development, and remain in touch with my clinical supervisor, Lisa Shepherd, who encouraged me to undertake the Masters Level Module in Endocrine Nursing.

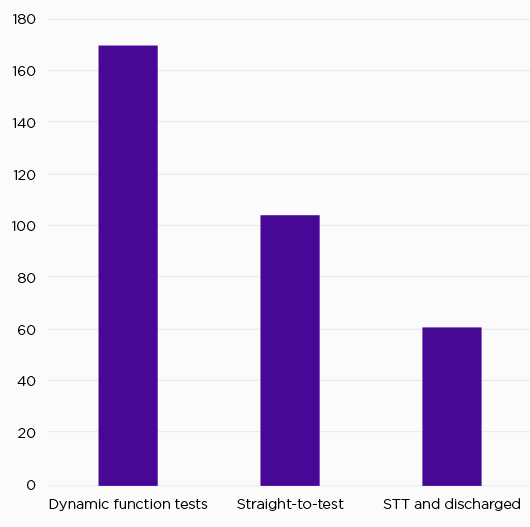
Figure 3. Dynamic function tests, straight-to-test (STT) investigations and subsequent nurse discharges, 2024.
LEARNING TO JUGGLE
My half-time share with diabetes has meant that I could continue in the lead nursing role for inpatient care. This, on occasions, has been quite puzzling for staff who sought an inpatient consultation on the day I was wearing the endocrine hat. Conversely, when there are deadlines looming or reports to consider, something (and it’s usually endocrine time) has to give.
The diversity in my current position means there are unlimited opportunities for me to learn from and share experiences with coworkers. I remain in awe of my very knowledgeable consultant colleagues who have to wear various hats, sometimes more than one hat at the same time! I enjoy the mixture of acute care and outpatient activity that my current, occasionally hectic, job provides.
Anecdotally, there may be an increase in dual roles. Discussion with my colleagues has indicated that, as well as my role in Bolton, examples of services adopting this dual-role approach, covering both diabetes and endocrinology, may be found in Northumbria, Shrewsbury and Telford. Possible motives could be financial, rather than employing a full-time endocrine specialist nurse, or taking a more considered approach to cross-cover services or increase professional development. There is little information within the literature with regard to dual roles and responsibilities, and how this may impact service provision. Further research or questionnaires would be welcomed.
AMY GLOVER
Specialist Nurse, Diabetes and Endocrinology, Royal Bolton Hospital
FURTHER READING
NHS England 2025 Hospital Outpatient Activity 2013–14 and 2018–19 https://digital.nhs.uk/data-and-information/publications/statistical/ hospital-outpatient-activity.
Wass J & Lansdown M 2021 Endocrinology GIRFT Programme National Specialty Report https://www.gettingitrightfirsttime.co.uk/wp-content/uploads/2021/09/EndocrinologyReport-Aug21o-NEW.pdf.
Discover our training and resources for nurses



{kind=link}
{kind=link}
{kind=link}