The skeleton is not traditionally considered a common site for diabetes complications, yet people with diabetes – both type 1 (T1D) and type 2 (T2D) – face a significantly higher risk of fragility fractures. The increase in fracture risk should be addressed along with the other complications of diabetes.

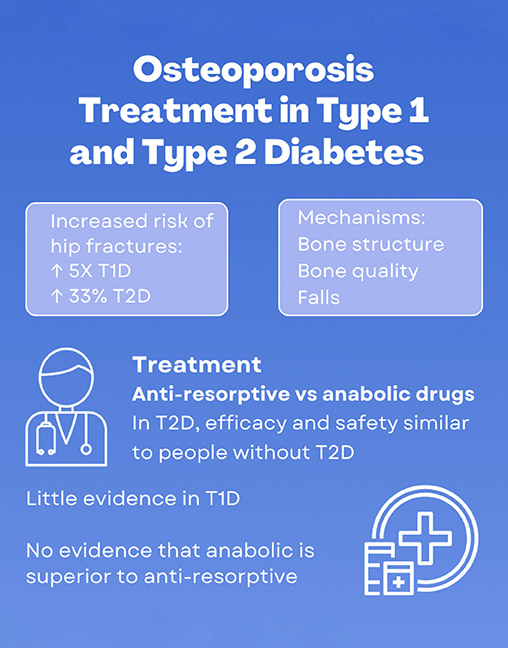
Figure. The increased risk of fragility fractures in both T1D and T2D highlights the need for greater attention to bone health. Reproduced under CC BY 4.0 licence from Vilaca T & Eastell R 2023.10 ©2023 The Authors
INCREASED FRACTURE RISK IN DIABETES
The risk of fractures is notably higher in both forms of diabetes, although the extent differs between T1D and T2D. For instance, individuals with T1D have a fivefold increase in the risk of hip fractures compared to people without diabetes. In T2D, the risk is around 30% higher. Similarly, the risk of non-vertebral fractures is doubled in T1D and 20% higher in T2D.1
In T2D, the risk is even more pronounced for those who have had diabetes for a more extended period or who are using insulin.1 However, insulin itself is not the culprit behind the increased fracture risk, as it is anabolic to bone, promoting bone formation. Instead, the heightened risk reflects the more severe nature of diabetes in these individuals.
BONE MINERAL DENSITY AND THE DIABETES PUZZLE
Bone mineral density (BMD) is a critical measure of bone strength and is commonly used to predict fracture risk. Interestingly, studies show that people with T1D often have slightly lower BMD than expected, but this reduction doesn’t fully explain the increased risk of fractures.2 This suggests that other factors are at play in increasing the risk of fractures in T1D.
The situation in T2D is even more intriguing. On average, individuals with T2D have a higher BMD than people without diabetes. Yet, despite this apparent advantage in bone density, the fracture risk is still elevated. It seems that BMD does not fully capture the effects of diabetes on bone health.2 However, bone density still predicts fractures in this population, as a relationship between fracture risk and BMD is observed. People with T2D have the same risk of fractures as people without diabetes, with a T-score (a measurement of BMD) 0.5 points lower.3 For example, a woman with diabetes and a T-score of –2.0 has the same risk of fractures as a woman without diabetes with a T-score of –2.5. This indicates that diabetes affects bone in ways beyond just density.
THE COMPLEX FEATURES ASSOCIATED WITH FRACTURE RISK IN DIABETES
The elevated fracture risk in diabetes is multifactorial, involving both skeletal and extra-skeletal factors.
Bone quality
Changes in bone microarchitecture (how bone tissue is organised on a microscopic level) have been observed in T1D and T2D.4,5 Hyperglycaemia promotes the accumulation of advanced glycation end products (AGEs), proteins or lipids that become glycated due to high blood sugar. Haemoglobin A1c, which is used to diagnose and monitor diabetes, is an example of an AGE. The process also affects bone collagen, and evidence suggests this could affect the protein’s properties, resulting in stiffer, more brittle bones that are prone to fractures.6
Fall risk
People with diabetes also face a higher risk of falls, which contributes to the fracture risk. Factors like poor balance, neuropathy (nerve damage) and vision problems are common in diabetes and increase the likelihood of falls. Episodes of hypoglycaemia, which can cause dizziness and confusion, also contribute to falls.6
Medications
Some medications used to treat diabetes can have negative effects on bone health. For example, thiazolidinediones (glitazones) are known to increase fracture risk. Some studies suggested that SGLT2 inhibitors lead to an increased risk of fractures, but this was not observed in all clinical trials.6
THE ROLE OF BONE TURNOVER
Bone turnover, the continuous process of bone resorption (breaking down) and formation, is essential for maintaining bone strength. In diabetes, most studies suggest that bone turnover decreases, as indicated by lower levels of bone turnover markers compared with people without diabetes.7
MANAGING BONE HEALTH IN DIABETES
Given the unique challenges diabetes poses to bone health, a proactive approach to managing fracture risk is essential.
Importance of glycaemic control
First and foremost, maintaining appropriate glycaemic control is a crucial aspect of managing bone health in diabetes. Good glycaemic control reduces the risk of hypoglycaemic episodes, and the development of diabetic complications, which in turn decreases the likelihood of falls. Additionally, better blood sugar control helps limit the formation of AGEs, thereby preserving bone quality. Over time, these efforts can reduce fracture risk and improve overall bone health.
Lifestyle interventions for bone health
Despite the presence of diabetes, basic bone health strategies remain vital:
• Calcium and vitamin D: Ensuring adequate intake of calcium and vitamin D is fundamental for maintaining strong bones.
• Exercise: Weight-bearing exercises, such as walking or resistance training, help build and maintain bone density.
• Avoiding smoking and excessive alcohol: Smoking and heavy alcohol consumption are harmful to bone health and should be avoided.
OSTEOPOROSIS TREATMENT IN DIABETES
Understanding that individuals with diabetes tend to suffer fractures at a higher T-score than those without the disease is key. As a result, osteoporosis treatment should be considered at a higher threshold: specifically, when the T-score reaches –2.0, which is less severe than the typical cutoff of –2.5 for people without diabetes.8
Current evidence suggests that osteoporosis treatments, such as bisphosphonates and anabolic therapies, are effective for people with T2D.9 Less evidence is available in T1D, but osteoporosis medications also seem efficacious and safe for these individuals. There is no clear indication that one medication or class of drugs is superior to another in this population.10
CONCLUSION: PROACTIVE BONE HEALTH IN DIABETES
Although the skeleton is not typically the first area of concern in diabetes management, the increased risk of fragility fractures in both T1D and T2D highlights the need for greater attention to bone health.
Effective glycaemic control, lifestyle interventions, early screening and appropriate treatment thresholds are essential tools in reducing the risk of fractures and preserving bone strength in people with diabetes. By addressing these issues head-on, we can help ensure that patients with diabetes won’t face fragility fractures as an extra complication of this disease.
TATIANE VILACA
Clinical Research Fellow, University of Sheffield
RICHARD EASTELL
Professor of Bone Metabolism, University of Sheffield
REFERENCES
1. Vilaca T et al. 2020 Bone https://doi.org/10.1016/j.bone.2020.115457.
2. Vestergaard P 2007 Osteoporosis International https://doi.org/10.1007/s00198-006-0253-4.
3. Schwartz AV et al. 2001 Journal of Clinical Endocrinology & Metabolism https://doi.org/10.1210/jcem.86.1.7139.
4. Vilaca T et al. 2021 Journal of Bone & Mineral Research https://doi.org/10.1002/jbmr.4271.
5. Walle M et al. 2022 Current Osteoporosis Reports https://doi.org/10.1007/s11914-022-00755-6.
6. Napoli N et al. 2017 Nature Reviews Endocrinology https://doi.org/10.1038/nrendo.2016.153.
7. Hygum K et al. 2017 European Journal of Endocrinology https://doi.org/10.1530/eje-16-0652.
8. Ferrari SL et al. 2018 Osteoporosis International https://doi.org/10.1007/s00198-018-4650-2.
9. Vilaca T & Eastell R. 2024 Current Osteoporosis Reports https://doi.org/10.1007/s11914-023-00833-3.
10. Vilaca T & Eastell R 2023 JBMR Plus https://doi.org/10.1002/jbm4.10838.


{kind=link}