Weight loss through calorie restriction, anti-obesity medications or bariatric surgery (BS) drives multiple health benefits. However, it has long been known that accelerated weight loss is linked to bone loss and resultant fractures. In the ‘Look AHEAD’ study, participants randomised to intensive lifestyle intervention experienced an average weight loss of 6% over a median time of 9.6 years. This degree of weight loss was associated with 39% increased risk of fragility fractures spanning 11 years, compared with a control group who only lost 3.9%.1
The Roux-en-Y gastric bypass (RYGB) and sleeve gastrectomy (SG) are the most common procedures in the UK and result in superior weight loss compared with lifestyle intervention and/or anti-obesity medications, typically between 20 and 35%. It is therefore not surprising that BS appears to have a substantial negative impact on bone health.
CURRENT UNDERSTANDING OF THE IMPACT OF BS ON BONE
In a study where participants were followed for 5 years after RYGB, there was a significant fall in bone mineral density (BMD) at both the spine (>5%) and the hip (>10%), with the greatest loss occurring within 2 years of surgery.2 However, of particular concern was the ongoing progressive fall in BMD at these sites beyond 2 years, despite stabilisation of weight.
Markers of bone resorption (serum levels of CTX (C-terminal telopeptide of type 1 collagen)) are increased within days after BS; they peak at around 1–2 years, with increases of between 50 and 300%, and remain elevated years after surgery. Bone formation markers (P1NP (procollagen type 1 N-terminal propeptide)) are also elevated, but to a lesser extent than CTX, resulting in net bone loss.
Furthermore, measures of bone microarchitecture (such as cortical porosity), which are important additional determinants of bone strength, are negatively impacted after BS.2
Collectively these detrimental impacts result in up to a twofold increase in fracture risk.3
NOT ALL THE BONE EFFECTS OF BS ARE EQUAL
Current data suggest that different types of BS impact bone health to varying degrees. Although SG leads to significant increases in CTX and P1NP, coupled with clinically significant drops in BMD, these changes are greater after RYGB.4
Consistent with this, an increased risk of major osteoporotic fractures (hazard ratio 1.7 over controls with obesity) has been observed after RYGB, but not after SG or gastric banding (GB), in a large, population-based, French study of over 80,000 participants, followed over 5 years.3
The jury is still out on whether the newer and most performed form of BS in the UK – the SG – leads to increased fracture risk. What is becoming clear is that fracture risk is increased following malabsorptive procedures, and this risk seems to emerge as early as 2 years postoperatively.5
POSSIBLE THEORIES TO EXPLAIN BONE LOSS AFTER BS

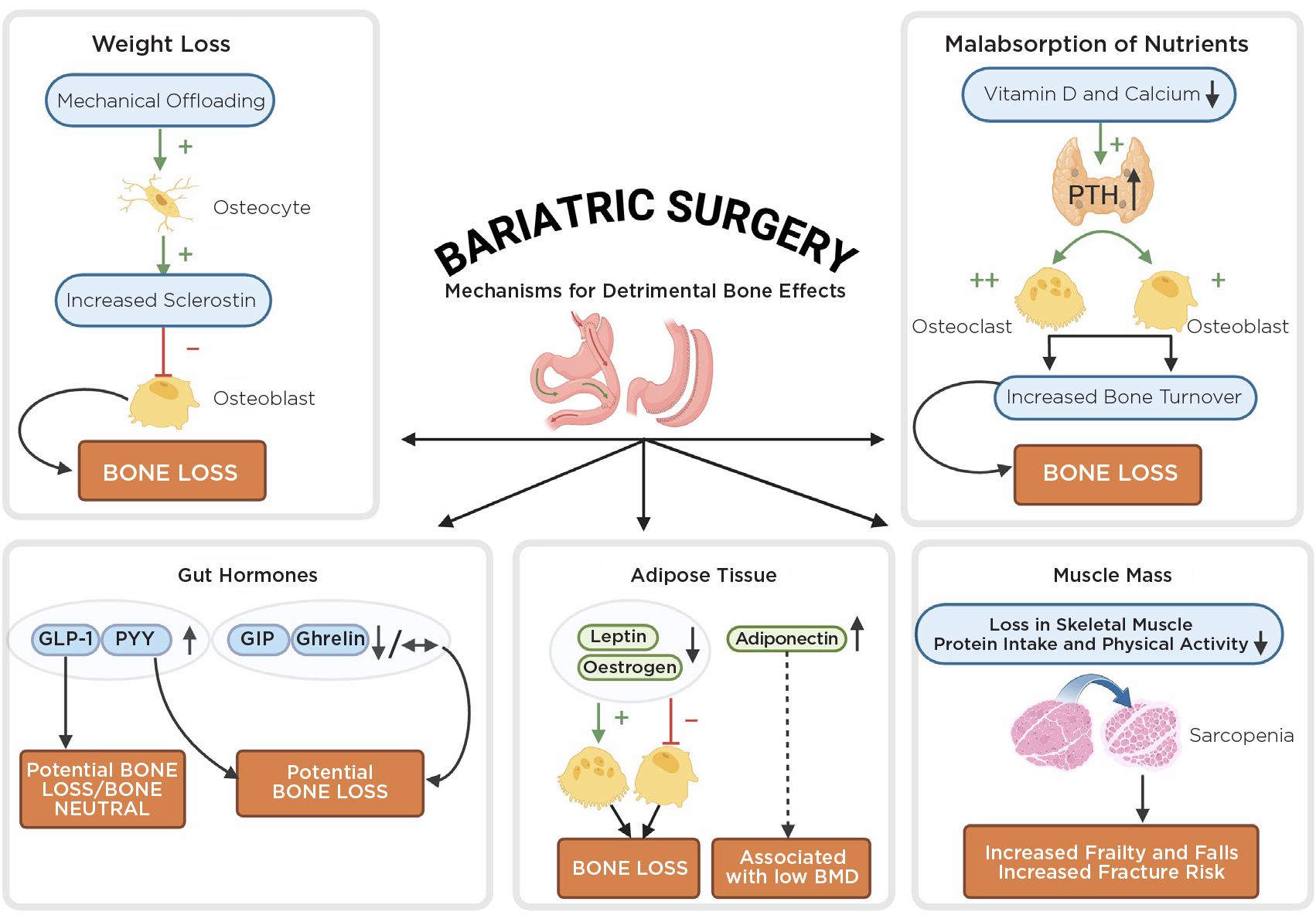
Figure. Possible theories to explain bone loss after bariatric surgery. PTH, parathyroid surgery; +, stimulate; –, inhibit. Created using BioRender.
The Figure illustrates potential mechanisms for detrimental bone effects.
The notion of mechanical ‘offloading’ of the skeleton, with weight loss resulting in bone loss, is a popular concept. Astronauts, for example, can lose up to 2% in BMD per month while in space.6 A positive correlation between weight loss and bone loss was observed in some but not all studies. Interestingly bone loss at the hip tends to be more extensive than at the spine. This is probably due to the weight-bearing hip bone being more susceptible to the detrimental effects of offloading. However, gradual bone loss continues beyond 2 years, despite stabilisation in weight loss or even a slight weight regain in some. This infers that other mechanisms are at play.
RYGB is associated with malabsorption of nutrients that are key for bone health. Vitamin D levels are generally suboptimal in members of the population who have obesity, and vitamin D deficiency/insufficiency can be further exacerbated after surgery due to malabsorption. In addition, calcium absorption is impaired after both SG and RYGB.7 In the latter, this relates to the bypassed proximal gut and reduced gastric acid production. The ensuing secondary hyperparathyroidism results in increased bone turnover, primarily bone resorption. Indeed, secondary hyperparathyroidism is highly prevalent, affecting approximately 50% of the population that has undergone BS at ≥5 years.8
The direct impact of gut hormones on bone is also important and an emerging area of study. Post-prandial levels of glucagon-like peptide-1 (GLP-1) and peptide YY (PYY) are substantially elevated after RYGB and SG, but not after GB. PYY has been shown to have negative effects on bone in rodent studies, primarily through suppression of osteoblastic activity.9
The impact of GLP-1 on human bone is less clear, especially when given at supraphysiological levels. A neutral effect on bone has been suggested but, worryingly, two recent trials reported reductions in hip/spine BMD at 1 year in participants with obesity but not diabetes, who were treated with semaglutide and liraglutide.10,11 The post-bariatric hormonal milieu is complex, with other notable changes in ghrelin, glucose-dependent insulinotropic polypeptide (GIP), adiponectin and leptin, all capable of exerting distinct effects on bone.
WHAT CAN WE DO?
Bariatric surgery is increasingly being recognised as a risk factor for bone health. The current British Obesity and Metabolic Surgery Society guidelines advocate for higher daily intakes of vitamin D (2000–4000IU with target levels >75nmol/l) and calcium (1200–1500mg).12
Other strategies include incorporating regular physical activity, especially strength training, while ensuring adequate intake of protein. However, these strategies can attenuate but not fully prevent bone and muscle loss after BS.13
What is less clear is who should be screened for low BMD prior to BS. Given the potential detrimental impacts on bone, it would be advisable for patients to have a fracture risk assessment (e.g. using FRAX®) before BS. Those identified to be at high fracture risk should undergo dual energy X-ray absorptiometry, with consideration of bone-specific (osteoporosis) therapies and close BMD monitoring after surgery.
It should be noted that there are no current data on the efficacy of standard bone-specific agents following BS, although a couple of studies are in progress (NCT04087096, NCT04742010). Parenteral agents (zoledronate, denosumab) are preferred treatment options after BS, as oral bisphosphonates are associated with increased risk of acid reflux and anastomotic ulceration. However, low vitamin D levels and hypocalcaemia are not uncommon and pose a major challenge for the safe administration of zoledronate or denosumab.
Those at a very high fracture risk or with a history of fragility fractures should ideally be managed in a specialised endocrine bone clinic that has expertise in this area.
PREESHILA BEHARY
Consultant Endocrinologist and Honorary Clinical Senior Lecturer, Department of Endocrinology, Imperial College Healthcare NHS Trust, London, and Section of Endocrinology and Investigative Medicine, Imperial College London
ALEX COMNINOS
Head of Endocrine Bone Unit, Department of Endocrinology, Imperial College Healthcare NHS Trust, London, and Section of Endocrinology and Investigative Medicine, Imperial College London
REFERENCES
1. Johnson KC et al. 2017 Journal of Bone & Mineral Research https://doi.org/10.1002/jbmr.3214.
2. Lindeman KG et al. 2018 Journal of Clinical Endocrinology & Metabolism https://doi.org/10.1210/jc.2018-01496.
3. Paccou J et al. 2020 Journal of Bone & Mineral Research https://doi.org/10.1002/jbmr.4012.
4. Hofsø D et al. 2021 Journal of Clinical Endocrinology & Metabolism https://doi.org/10.1210/clinem/dgaa808.
5. Saad RK et al. 2022 Osteoporosis International https://doi.org/10.1007/s00198-021-06206-9.
6. Orwoll ES et al. 2013 Journal of Bone & Mineral Research https://doi.org/10.1002/jbmr.1948.
7. Wu KC et al. 2023 Journal of Clinical Endocrinology & Metabolism https://doi.org/10.1210/clinem/dgac579.
8. Gao Z et al. 2022 Obesity Reviews https://doi.org/10.1111/obr.13488.
9. Schiellerup SP et al. 2019 Frontiers in Endocrinology https://doi.org/10.3389/fendo.2019.00075.
10. Jensen SBK et al. 2024 JAMA Network Open https://doi.org/10.1001/jamanetworkopen.2024.16775.
11. Hansen MS et al. 2024 eClinicalMedicine https://doi.org/10.1016/j.eclinm.2024.102624.
12. O’Kane M et al. 2020 Obesity Reviews https://doi.org/10.1111/obr.13087.
13. Muschitz C et al. 2016 Journal of Bone & Mineral Research https://doi.org/10.1002/jbmr.2707.


{kind=link}