Imagine you, your child, or someone else you care about is diagnosed with a brain tumour. They may present very unwell, with neurological deficits due to a space-occupying lesion. They may have a suprasellar mass presenting with endocrine issues such as arginine vasopressin deficiency (cranial diabetes insipidus) and hypopituitarism. They may complain of loss of vision. It’s all very stressful. And then imagine there is hydrocephalus, ventriculo–peritoneal (VP) shunt insertion, a neurosurgical operation, radiotherapy and possibly chemotherapy. That is all pretty traumatic. We describe this in our service as an acquired brain injury – not a single incident, as in a road traffic accident for example, but multiple and progressive injuries to the brain.
THE ROLE OF THE ENDOCRINOLOGIST
In endocrinology, we are asked to help with the care of people who have undergone treatment for brain tumours, often in childhood.
It is crucial to ask for the field of radiotherapy (especially with the advent of proton beam therapy), in order to know the dose that the hypothalamus, pituitary and thyroid have received. If the hypothalamus/pituitary is not affected, then this cohort is better served in a late effects neuro-oncology service. These are few and far between, especially considering that more and more people live with and beyond a cancer diagnosis. The thyroid is very sensitive to radiation and the neck should be palpated annually in anyone who has had posterior fossa, brain stem or craniospinal irradiation where the thyroid receives some radiotherapy.
Different hormone axes are affected at different doses of radiotherapy (including proton beam therapy) when the hypothalamus/pituitary is in the treatment field:
- Growth hormone defiency can occur after 10–15Gy and occur up to 15 years after treatment. The time to development of deficiency reduces with higher doses, down to around 12 months after 60Gy or more.
- Impact upon follicle-stimulating hormone and luteinising hormone means that precocious puberty can result from doses as low as 15–20Gy.
- Thyrotrophin (TSH) deficiency is less common and predominantly occurs after 30Gy or more.
- Adrenocorticotrophin (ACTH) deficiency is also less common and predominantly occurs after 30Gy or more.
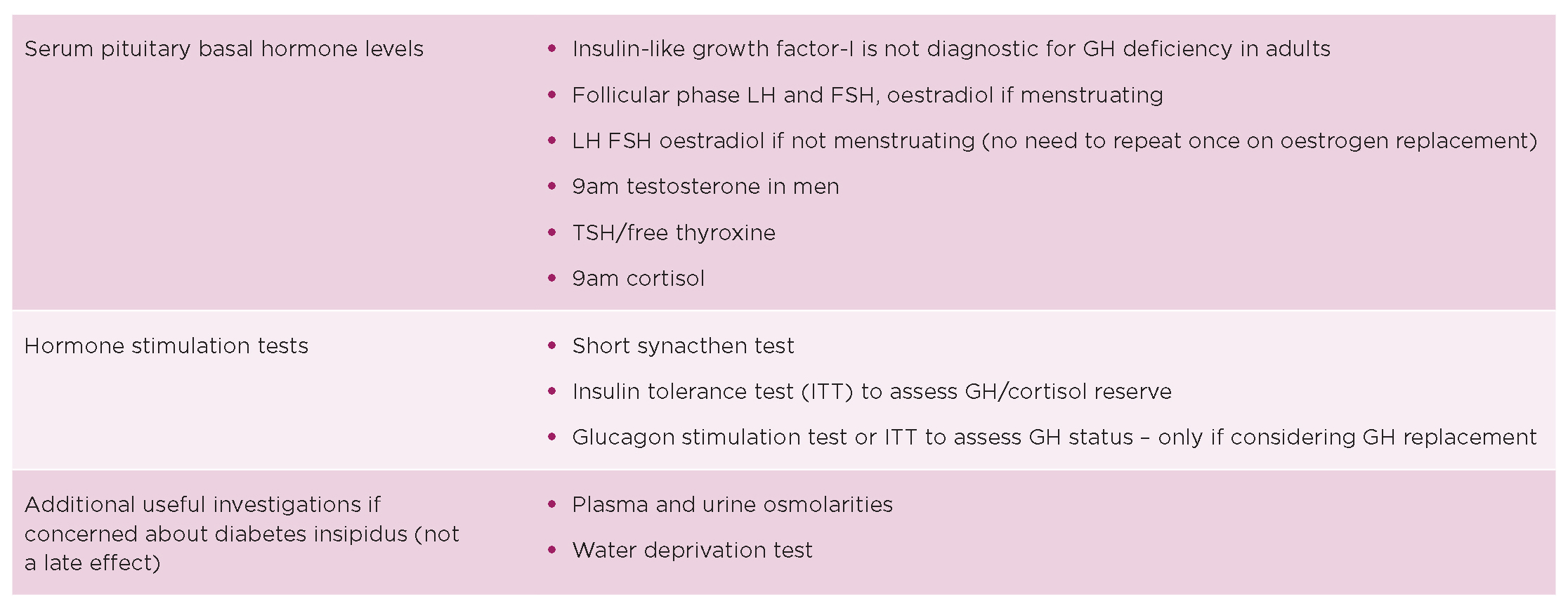
In the case of ACTH, is it important to determine if exogenous glucocorticoid was around at the time of testing for adrenal insufficiency, and that there has been an appropriate test performed, before confirming this important diagnosis. There are issues around assays, cut-offs and dynamic tests used. The glucagon test, for example, performs badly as a test for ACTH/cortisol production. The table shows a suggested testing strategy.
The highest risk of pituitary dysfunction comes in the first 10 years. Our strategy at University College London Hospitals is a dynamic test if growth hormone (GH) is being considered 6–12 months after completion of treatment, then a 9am blood test annually for 10 years unless the clinical picture changes. GH testing frequency is harder to determine: my strategy is roughly 5 years for two dynamic tests as determined by adult GH deficiency assessment (AGDHA; if over 25) and discussion with the patient. While GH is not licensed in active malignancy, to date there are no safety concerns in this cohort. The main risk is of type 2 diabetes in those with additional risk factors.

Table. Suggested strategy for endocrine testing. FSH, follicle-stimulating hormone; LH, luteinising hormone.
NEUROLOGICAL IMPACT
As well as affecting hormone production, radiotherapy can affect neurones and dendritic connections, and result in issues with neurocognitive function, or issues with higher executive functions, such as learning, memory and processing speed of the brain. This is more apparent the younger the person is having radiotherapy, and is associated with the volume of brain affected, and the site of neurosurgery. For example, a cohort of young people in our care have had whole brain irradiation (e.g. for medulloblastoma), receiving 40Gy, and have significant early memory loss in their 30–40s. Memory loss can make it difficult to manage aspects of hormone replacement, in particular desmopressin and glucocorticoid replacement, and remembering sick day rules. Radiotherapy can affect blood vessels in the brain; the risk of stroke increases, and rises further after about 20 years. We don’t know the mechanism for this or how to manage it. It is important to focus on healthy eating and exercise, and monitoring other cardiovascular risk factors such as lipids, glycated haemoglobin and blood pressure. St Jude’s CVS Risk Calculator may also be helpful in decision making.
Neurosurgery can be life-saving. You don’t need me to describe how this is traumatic to the brain. Hydrocephalus, often the first presentation of a primary brain tumour, causes pressure in the brain, managed with a VP shunt or Omyaya reservoir. Shunts can block, malfunction and, rarely, get infected, so needing to be removed. An often forgotten, important part of care for this patient group is ensuring that they are known to a hydrocephalus service, so they can have a shunt check as needed.

Brain tumours and their treatment can cause wide-ranging stress and trauma. Credit: shutterstock
How all of this can affect people in terms of neurocognitive function and also mental health spans a huge spectrum. It is common to see young people with anxiety, and there are a number of people with mental health diagnoses, such as psychosis and severe depression. Referrals for talking therapies, neuropsychology or psychiatry should be considered.
IDENTIFYING SUPPORT SERVICES
One of the challenging aspects of care is linking to services that can support this cohort, as services are not commissioned, and many are community-based and can be difficult to access, or are non-existent. Part of the jigsaw that is helpful for patients is a documented educational assessment, documenting if the young person has a learning disability, and ensuring young people are linked with adult learning disability teams prior to transition to adult services. Patient support groups such as Trekstock, Macmillan, Ellen MacArthur Trust, Children’s Cancer and Leukaemia Group, Headway, Success and Brainstrust can offer support. It is important to know if there is a lasting power of attorney for health in place for those with significant brain injury, and Citizens Advice and local Council adult learning disability teams can be a source of information for parents and carers. Macmillan has support to navigate the benefits system.
Neurocognitive function testing should be considered where these may be a concern, as strategies can be offered linking to occupational therapy and vocational therapy. Young people may need support navigating the education system and going to university, along with support in the workplace.
Fatigue is a very common. It is rarely related to endocrine deficits if they are appropriately replaced. It is usually related to the acquired brain injury itself affecting capacity of neurocognitive function. Links with neurology and brain injury teams can be helpful to access support and discuss strategies, such as pacing activities and good sleep patterns. Some people have access to fatigue management services run by occupational therapy and, if so, a referral here can be helpful.
There is a lot to consider – stress and trauma coming from both tumours and treatments. Endocrine deficits should not be missed, and we should screen for long term impacts of treatments appropriately and pragmatically. Multidisciplinary working is key, with non-medical interventions often being the most important for quality of life. There remains a gap between services needed and what is available.
HELEN SIMPSON
Deputy Clinical Lead Diabetes and Endocrinology, UCLH NHS Foundation Trust
FURTHER READING
Children’s Cancer and Leukaemia Group Late Effects Factsheets.
Gebauer J et al. 2019 Endocrine Reviews https://doi.org/10.1210/er.2018-00092.
Headway Fatigue after Brain Injury.
International Late Effects of Childhood Cancer Guideline Harmonization Group.
Late Effects Special Edition 2022–2023 Endocrine Connections https://ec.bioscientifica.com/page/lateeffects/late-effects-special-issue.
Macmillan Endocrine Late Effects Guide.
Office of the Public Guardian Lasting Power of Attorney.
Stochholm K & Kiess W 2018 Clinical Endocrinology https://doi.org/10.1111/cen.13502.




{kind=link}
{kind=link}