John Honour is an Honorary Senior Research Associate at the Institute for Women’s Health at University College London, and was previously a Consultant Clinical Scientist in Clinical Biochemistry at UCLH and Head of the Specialist Service for Steroid Endocrinology. His long career has focused on steroid analysis in the context of understanding disease, with an interest in the impact of bacteria on steroid metabolism.
MY EARLY CAREER
I came to a career in endocrinology in 1972, when I joined Cedric Shackleton at the MRC Clinical Research Centre (CRC) in Harrow. Cedric had just started to use capillary column gas chromatography to examine steroids in the urine of patients with adrenal disorders. The stationary phase was a wall coating of silicone polymer on the glass column; this was held in place with heat-shrink polytetrafluoroethylene. The capillary column was 30m long and 0.1cm wide, and replaced the original glass columns (these were often 4m long and 0.5cm in diameter, filled with diatomaceous earth coated with stationary phase). Glass capillaries were replaced with fused silica which was more robust. In 1978, the CRC team produced an atlas of the steroid profiles seen to that time. I suppose we can say this was near the start of metabolomics.
The Clinical Chemistry Department was equipped with a magnetic sector mass spectrometer that almost filled the room, and was probably 20 times bigger than current gas chromatography–mass spectrometry (GC–MS) systems. One important study for me was to perform urinary steroid profile analysis on samples from a patient whom we found to have a rare form of congenital adrenal hyperplasia from 17-hydroxylase deficiency. The steroids we found were metabolites of corticosterone and progesterone, but as well as hepatic metabolites there were products of an enterohepatic circulation with bacterial transformation, notably 21-dehydroxylation. Although this was many years before the universal use of the microbiome that we see today, the bacterial process had been described by Jan Sjövall and Håkan Eriksson in rats in 1965–1972. Some of this information was useful in interpretation of the patient data.
CLINICAL RESEARCH AND PRACTICE

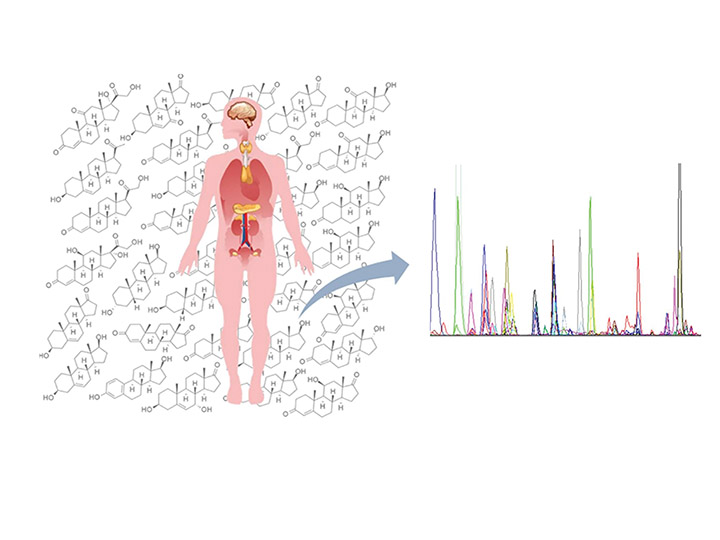
Figure 1. Seeing through the ‘chicken wire’.
Over the next 40 years at the CRC, Middlesex Hospital and University College London Hospital, I used GC–MS in clinical research. From clinical collaboration, I learnt the need to explain steroid results to clinicians and to act promptly for sick patients. On ward rounds, I saw sick children with adrenal disease and encountered the parents of children who could not be sure of the sex of their baby.
Some clinicians could not see the steroid path beyond the ‘chicken wire’ (see Figure 1), so there was a need to explain the process of steroidogenesis and metabolism.
Over the years in clinical practice, I encountered patients with almost every known disorder of the adrenal cortex and differences in sexual development. I was involved in clinical research around assisted fertility, polycystic ovary syndrome, preterm infants, osteoporosis, adrenarche, vegetarian diets, hypertension, asthma, AIDS/HIV and septic shock.
For several years, I acted as an expert witness in cases of drug abuse in sport, many due to nandrolone that was found to be in nutritional supplements. The defence of Diane Modahl was based on the demonstration of testosterone formation by bacteria, which acted on steroids in the urine when the sample was left outside the closed laboratory in Lisbon in Portugal, over a weekend in mid-summer. Samples don’t get treated like that in the clinical setting.
ADVANCES IN TECHNOLOGY

Figure 2. Launching my book among friends.
Towards the end of my career, immunoassay was being discredited thorough lack of specificity and liquid chromatography coupled with mass spectrometry (LC–MS) was becoming popular for steroid analysis. One important attraction was that the steroids did not need to be chemically stabilised for high temperature GC analysis, making the technique more suitable for clinical laboratories. Even steroid conjugates could be analysed directly.
The specificity of LC–MS was improved further by using tandem mass spectrometry (LC–MS/MS), which reflects two mass spectrometers but has three components. After ionisation of the steroid, a fragment ion in the first segment of the mass spectrometer is selected for collision-induced dissociation in stage two, and ions that are then produced are selected for detection in the third stage. Stable isotope-labelled internal standards are ideal. Steroid isomers need to be separated in the LC stage, and it is crucial to test for ion suppression or enhancement by compounds co-eluted into the MS.
A LOCKDOWN PROJECT
In 2021/2022, after treatment for malignant melanoma, I was in the Government-advised shielding group due to the COVID-19 pandemic. I made use of the time at home to write up my work experience.

Figure 3. My lockdown project, to answer questions around steroids in the laboratory and clinic. © 2023 Elsevier Inc.
In September 2023, this was published as Steroids in the Laboratory and Clinical Practice1 (Figures 2 and 3). No such book had been published in this detail since Steroid Hormones2 by David Gower in 1979, but much had changed since then. The book ended up as a 988-page monster, covering basic chemistry, methods for steroid analysis, and clinical application of steroids. There are more than 730 figures and 120 tables to enhance comprehension of the wide-ranging and often complex material. I hope this labour of love will become the ‘go to’ for answers to questions around steroids in the laboratory and clinic for pathologists, laboratorians, endocrinologists, analytical/clinical chemists and biochemists.
Steroid hormones and their metabolites, once considered inert, are now all known to play important pivotal functional roles. My professional journey provided me with unmatched broad experiences of steroids in clinical practice that enabled me to write the book for others to benefit.
THE IMPORTANCE OF COLLABORATION
I should acknowledge the many staff in my laboratory and the clinicians locally and around the world with whom I had the privilege to collaborate scientifically, for the benefit of many patients. I must emphasise the need for a dialogue between the parties, because aspects of the investigations are becoming more complicated in different ways for each, so both will benefit from the exchange of information and knowledge.
It’s been a pleasure to walk a memory lane of my career and membership of the Society for Endocrinology since around 1975, and the many fruitful meetings with colleagues for exchange of ideas, banter and a few beers.
REFERENCES
- Honour JW 2023 Steroids in the Laboratory and Clinical Practice, 988 pp. Elsevier.
- Gower DB 1979 Steroid Hormones, 116 pp. Yearbook.



{kind=link}
{kind=link}
{kind=link}