The mortality rate in patients with adrenal insufficiency is higher than in the general population, mainly because of an increased risk of cardiovascular death. This may be due to excess steroid exposure, or replacement regimens that are uncoupled from the normal physiological cortisol profile.1
Adrenal insufficiency requires careful management to prevent life-threatening adrenal crises. ‘Sick day rules’ recommend increased glucocorticoid doses during physiological stress, such as illness or surgery. However, the evidence supporting the optimal glucocorticoid dose and duration is lacking. A better understanding of stress effects on the hypothalamic-pituitary-adrenal (HPA) axis is needed to inform the development of future guidelines. Additionally, the evolutionary advantage of elevated serum cortisol levels during stress may no longer apply in a world with antibiotics, vaccinations and intensive care units. Simply doubling or tripling the dose of hydrocortisone when the patient may have been exposed to minor ‘stress’ may be harmful, particularly if this is frequent.
“ ‘Sick day rules’ recommend increased glucocorticoid doses during physiological stress, such as illness or surgery. However, the evidence supporting the optimal glucocorticoid dose and duration is lacking.”
The control of the HPA axis is poorly understood. While there are circadian and ultradian rhythms, the exact mechanism by which the hypothalamus modulates cortisol levels is unknown.1 Corticotrophin-releasing hormone (CRH) stimulates adrenocorticotrophin (ACTH), which then stimulates cortisol, with negative feedback at the level of the hypothalamus and pituitary. The regulation of hypothalamic CRH release is complex, involving stimulatory and inhibitory neural networks.
STRESS RESPONSE VARIABILITY
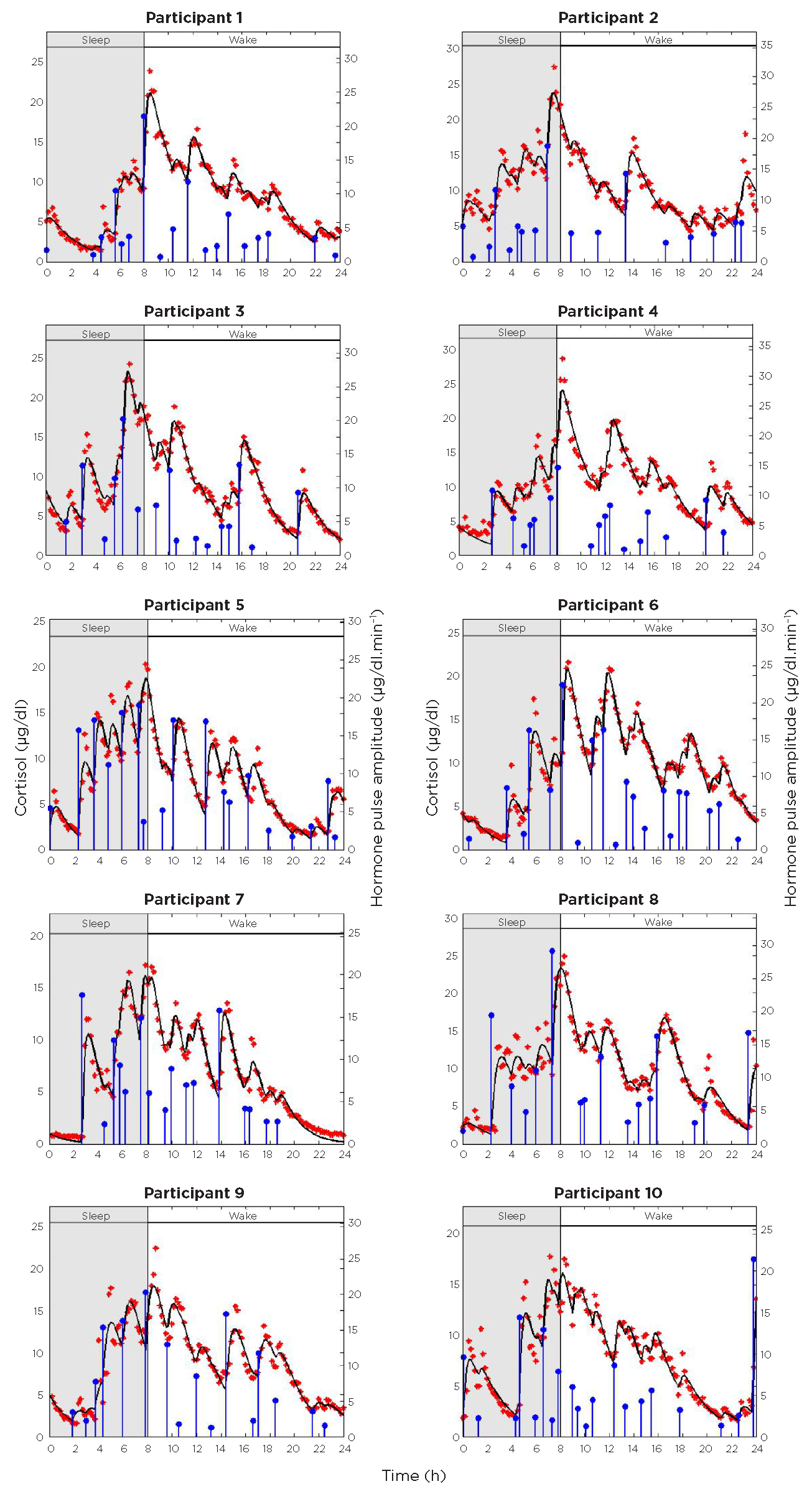
It is believed that ‘stress’ may cause an increase in activity of the HPA axis, although there is an extremely wide inter-individual variation in HPA responses to similar stress. Deconvoluted data of individual patients show enormous variability.2 Ten 24-hour serum cortisol profiles from adult females indicate that the adrenal gland produces cortisol in distinct bursts, superimposed on a circadian rhythm. Despite this episodic secretion, the overall cortisol concentration remains continuous but highly variable and unpredictable in each individual (Figure).

Figure. 24-hour serum cortisol profile in 10 individuals demonstrating wide variations between individuals. Reproduced under Creative Commons Attribution License from Faghih et al. (2) ©2014 The Authors.
The ‘sick day rules’ were suggested following the publication, in 1968, of the effects of surgery on cortisol levels in 40 individuals who were undergoing surgical procedures, such as gastrointestinal surgery, hysterectomy or hip osteotomy.3 The study noted wide variation in cortisol responses to the same surgery among different individuals, although the individual data were not provided.
Recent data show wide variation in cortisol responses among 93 euadrenal patients undergoing elective surgery.4 Despite the physiological stress of a cholecystectomy, some individuals demonstrated almost no rise in cortisol. The study categorised surgeries by severity: major/major+ (n=37), moderate (n=33) and minor (n=23). Peak serum cortisol concentrations ranged from 272 to 1066nmol/l after minor surgery and from 375 to 1452nmol/l after major surgery.
Surprisingly, ACTH levels are not responsible for the peri-operative rise in cortisol. Following cardiac surgery, there is a significant surge in both ACTH and cortisol levels. Even after ACTH levels return to baseline, cortisol remains elevated, which suppresses ACTH. This suggests an increase in adrenal sensitivity to ACTH.5
GLUCOCORTICOID DOSING DURING STRESS
Although we prescribe double or triple doses of glucocorticoids during times of stress,6 evidence of benefit is unclear, and it may be harmful in some cases. The interpretation of stress is highly variable. Evidence is difficult to obtain because, if there is a benefit, withholding increased glucocorticoids could be harmful. Understanding what type of ‘stress’ activates the HPA axis will help develop a more nuanced approach to sick day rules. Using extra glucocorticoids during sepsis might be harmful, given their immunosuppressive effects.7
A retrospective study by Hahner et al. documented 384 adrenal crises over 6092 patient-years, with an incidence rate of 6.3 crises per 100 patient-years, mainly triggered by gastrointestinal infections and fever. The incidence was unaffected by educational status, body mass index, glucocorticoid dose, dehydroepiandrosterone treatment, age at diagnosis, hypogonadism, hypothyroidism, or growth hormone deficiency.8 A follow-up prospective study involving 423 patients found a high prevalence of adrenal crises even among educated patients, with no other significant associations other than a history of crises.9 These studies suggest that patient knowledge and understanding of sick day rules have not improved patient outcomes.
The suggestion that steroid doses are doubled or tripled should refer to patients on replacement doses of prednisolone (2–4mg) or hydrocortisone (10mg+5mg+2.5mg). However, patients on higher, immunosuppressive doses for rheumatological conditions might double their prednisolone from 20 to 40mg, even though 20mg is already well above a typical stress dose.10
Others report that patients following sick day rules have better outcomes when they develop sepsis, but it’s important to understand that recovery associated with glucocorticoid use doesn’t necessarily mean that the glucocorticoid caused the improvement. Thus, septic hypotensive patients typically receive antibiotics and fluids first, and any progress seen after steroids might be due to these initial treatments or improved fluid management, rather than the steroids. If there is no immediate response to steroids, additional doses are given, and any eventual improvement is often mistakenly attributed to the glucocorticoid. This potential bias should be considered before attributing the improvement to the hydrocortisone. While many believe sick day rules are beneficial, there is limited evidence beyond self-assessment questionnaires, and publications often lack data on adrenal crisis frequency, hospitalisations and mortality rates.11
OPTIMISING DOSING STRATEGIES
Glucocorticoid dosing recommendations for adrenal insufficiency vary widely, indicating a lack of consensus on optimal strategies and underscoring the need for robust evidence to standardise practice. Current sick day rules, based on observational studies, physiological data and consensus, are widely recommended, but have not been proven to reduce the incidence of adrenal crises. Long term supraphysiological glucocorticoid doses may lead to weight gain, metabolic syndrome, muscle wasting and impaired immune response, and contribute to the increased mortality that we know occurs due to cardiovascular disease. The absence of high quality randomised controlled trials and standardised dosing protocols highlights the need for more research. Future studies should focus on optimising dosing strategies and using technology for real-time monitoring of cortisol levels to improve patient management during stress.12
ZIN HTUT
Clinical Research Fellow, Imperial College London
NIAMH MARTIN
Professor of Endocrinology and Consultant Endocrinologist, Imperial College London, Imperial College Healthcare NHS Trust
KARIM MEERAN
Professor of Endocrinology and Consultant Endocrinologist, Imperial College London, Imperial College Healthcare NHS Trust
REFERENCES
- Choudhury S et al. 2019 Clinical Endocrinology https://doi.org/10.1111/cen.13999.
- Faghih RT et al. 2014 PLoS One https://doi.org/10.1371/journal.pone.0085204.
- Plumpton FS & Besser GM 1969 British Journal of Surgery https://doi.org/10.1002/bjs.1800560315.
- Khoo B et al. 2017 Clinical Endocrinology https://doi.org/10.1111/cen.13439.
- Gibbison B et al. 2015 Critical Care Medicine https://doi.org/10.1097/CCM.0000000000000773.
- Bornstein SR et al. 2016 Journal of Clinical Endocrinology & Metabolism https://doi.org/10.1210/jc.2015-1710.
- Langouche L et al. 2023 Endocrine Reviews https://doi.org/10.1210/endrev/bnad021.
- Hahner S et al. 2010 European Journal of Endocrinology https://doi.org/10.1530/EJE-09-0884.
- Hahner S et al. 2015 Journal of Clinical Endocrinology & Metabolism https://doi.org/10.1210/jc.2014-3191.
- Sharma A et al. 2023 Endocrine Connections https://doi.org/10.1530/EC-23-0097.
- Burger-Stritt S et al. 2020 European Journal of Endocrinology https://doi.org/10.1530/EJE-20-0181.
- Upton TJ et al. 2023 Science Translational Medicine https://doi.org/10.1126/scitranslmed.adg8464.


{kind=link}