We are delighted to include this summary of the 2022 Early Career Prize Lecture (Clinical) given by Catherine Lovegrove at SfE BES 2022.
Through my research into kidney stone disease, I aim to improve our understanding of the genetic causes of this condition within the general population, and the care we offer patients, by providing better treatment and prevention strategies.
Kidney stone disease is a common condition, affecting approximately 1 in 5 men and 1 in 10 women by the age of 70 years. It accounts for over 85,000 hospital attendances per year in England.1,2 Half of people experiencing a kidney stone will have a second within approximately 10 years, and recurrent kidney stone disease is linked to an increased risk of chronic kidney disease.3,4 Despite the high prevalence of kidney stones, our understanding of the underlying environmental and genetic causes is incomplete, hindering our ability to effectively treat and prevent them.
RISK FACTORS FOR KIDNEY STONES
'Despite the high prevalence of kidney stones, our understanding of the underlying environmental and genetic causes is incomplete.'
Observational epidemiological studies suggest that obesity is a risk factor for kidney stones. Obesity is linked to metabolic syndrome, a cluster of diseases including central adiposity, hypertension, dyslipidaemia and impaired glucose tolerance, which have also been linked to kidney stone disease in observational studies.5,6 How adiposity and metabolic syndrome are associated with an increased risk of kidney stones is uncertain. However, postulated mechanisms include altered urine composition, altered serum biochemistry and systemic inflammation. I wanted to investigate how obesity and metabolic syndrome are linked to kidney stone disease, and used a technique called Mendelian randomisation, which aims to overcome some of the limitations that affect observational studies, including reverse causality and residual confounding.
Mendelian randomisation uses genetic variants, randomly inherited at conception, to assess the causal relationship between a risk factor and an outcome.7 An analogy is frequently made with a ‘genetic randomised control trial’. This comparison does not adequately capture the complexity involved in identifying causal relationships; however, it can be a useful illustration. Briefly, Mendelian randomisation uses genetic associations with a risk factor (often identified from genome-wide association studies) to generate exposure and control groups. The risk of an outcome in these genetically predefined groups is subsequently evaluated. The technique can also be employed with continuous variables.

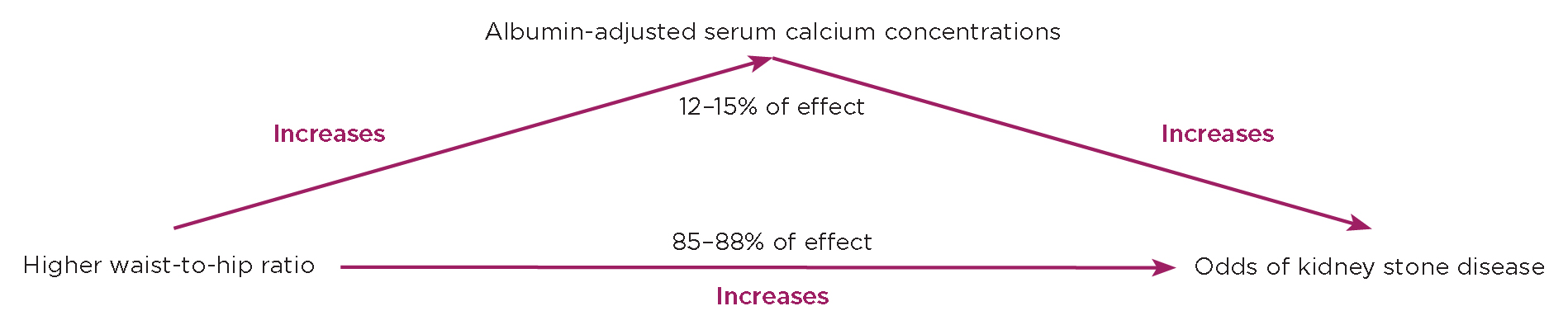
Figure. Higher waist-to-hip ratio has a causal effect to increase the odds of kidney stone disease, which is partially mediated via increasing serum calcium concentrations.
MY WORK FOR THE EARLY CAREER PRIZE
Using data from the UK Biobank and FinnGen studies, I was able to look for causal relationships between obesity and kidney stone disease.
First, with collaborators from the Nuffield Department of Population Health (University of Oxford), I confirmed that higher general adiposity (body mass index, BMI) and central adiposity (waist circumference, WC; waist-to-hip ratio, WHR) are independently associated with an increased risk of kidney stones in sex-stratified and combined-sex observational analyses in the UK Biobank.
Next, to facilitate Mendelian randomisation analyses, I performed a genome-wide association study of kidney stone disease in 8,504 cases and 388,819 controls in the UK Biobank, and meta-analysed these findings with data from the FinnGen study.8,9 I undertook Mendelian randomisation analyses and showed that an increase in BMI, WC and WHR of one standard deviation is associated with increased odds of kidney stone disease (odds ratio (OR) 1.36, 95% confidence interval (CI) 1.25–1.48; OR 1.35, 95% CI=1.07–1.71; OR 1.33, 95% CI=1.18–1.50 respectively). This supported the findings from observational analyses. Multivariable analyses indicated that general and central adiposity are independent risk factors for kidney stone disease and bi-directional analyses showed no effect of kidney stone disease on BMI, WC or WHR.
Having confirmed that increased adiposity causally increases risk of kidney stones, I wanted to identify the mechanisms underlying this finding. Therefore, I systematically evaluated the effects of serum and urinary biochemical phenotypes, components of metabolic syndrome and markers of systemic inflammation on the odds of kidney stone disease. I found that increasing albumin-adjusted serum calcium concentrations by 0.08mmol/l increases the odds of kidney stones by 48%, and that a higher WHR causally increases serum calcium concentrations independently of BMI (an increase in WHR of one standard deviation elevates serum calcium concentration by 0.12mmol/l, SE 0.02). Interestingly, higher BMI had no effect on serum calcium after adjusting for WHR. These findings suggest that central adiposity, but not general adiposity, increases risk of kidney stones via effects on serum calcium concentrations. Using mediation Mendelian randomisation analyses, I estimated that ~12–15% of the effect of higher WHR on increasing the odds of kidney stone disease arises from effects on serum calcium concentrations (see Figure).
I found no evidence that hypertension, dyslipidaemia, markers of glycaemic control, or systemic inflammation increases liability to kidney stones in Mendelian randomisation analyses. I did identify that type 2 diabetes may increase the odds of kidney stone disease. However, multivariable analyses with BMI and WHR indicated that this effect is probably confounded by co-existing adiposity.
IMPLICATIONS AND FUTURE WORK
My work highlights the importance of general and central adiposity as causal risk factors for kidney stone disease, and reports the novel finding that higher WHR increases serum calcium concentrations. This has implications for counselling patients to reduce their risk of kidney stones through lifestyle modifications, such as diet and exercise, and provides impetus to investigate the role of weight loss therapies to prevent kidney stones. Finally, these findings motivate research into how higher WHR increases serum calcium concentrations to identify novel therapeutic opportunities and translate results for patient benefit.
CATHERINE LOVEGROVE
MRC Clinical Research Training Fellow and Clarendon Scholar, Nuffield Department of Surgical Sciences, University of Oxford
The author is a urology trainee in the Thames Valley region, undertaking an MRC Clinical Research Training Fellowship and studying for a DPhil in Surgical Sciences at the University of Oxford, supervised by Dr Sarah Howles and Professors Dominic Furniss and Michael Holmes. This research has been published as Lovegrove CE et al. 2023 Journal of the American Society of Nephrology https://doi.org/10.1681/ASN.0000000000000238.
Find out more about Early Career Prize Lectures
REFERENCES
1. Abufaraj M et al. 2021 European Urology Focus https://doi.org/10.1016/j.euf.2020.08.011.
2. Jour I et al. 2022 BJU International https://doi.org/10.1111/bju.15728.
3. Zhe M & Hang Z 2017 Urolithiasis https://doi.org/10.1007/s00240-016-0938-x.
4. Lovegrove CE et al. 2022 BJU International https://doi.org/10.1111/bju.15522.
5. Ping H et al. 2019 BJU International https://doi.org/10.1111/bju.14805.
6. Masterson JH et al. 2015 Urolithiasis https://doi.org/10.1007/s00240-014-0719-3.
7. Davies NM et al. 2018 BMJ https://doi.org/10.1136/bmj.k601.
8. FinnGen 2024 FinnGen Research Project https://finngen.gitbook.io/documentation.
9. Kurki MI et al. 2023 Nature https://doi.org/10.1038/s41586-022-05473-8.



{kind=link}